What are Tension Headaches?
What are Tension Headaches?

Headaches are among the most prevalent healthcare disorders affecting North Americans. The most common type of headache is a tension headache. Tension-type headaches affect 30 – 80 % of the general population (women are 2x’s more likely to be afflicted) with the average individual experiencing tension headaches twice a month. Three percent of the population suffer from chronic daily tension headaches. Tension-type headaches are usually classified as either episodic or chronic based on the frequency. According to the International Headache Society (IHS), episodic tension headaches occur less than 15 days per month; whereas, chronic tension-type headaches occur more than 15 times a month, for at least six months.
Signs and Symptoms of Tension Headaches
Tension Headaches are characterized as a squeezing or vice sensation that presents bilaterally on the front, sides or top of your head. Patients with tension headaches tend to notice that their symptoms present later in the day, are associated with stressful events and affect a persons ability to concentration. Research has shown that the intensity of tension headaches increases with the frequency in which they present.
Tension headaches differ from migraines in that they do not present with neurological impairments, such as: vision, balance or strength deficits. Patients usually do not present with severe sensitivity to light/sound, nausea and vomiting.
Causes of Tension Headaches
There is no definitive cause or family predisposition for having tension-type headaches. Tension headaches are usually associated with inadequate rest, poor posture, emotional or mental stress, depression, fatigue and overexertion.
Suboccipitals and the Myodural Bridge
One proposed mechanism for the cause of tension-type headaches that has gained a lot of traction in recent years in the relationship between the suboccitipal muscles and a myodural bridge. Before we continue, let’s cover some basic anatomy.
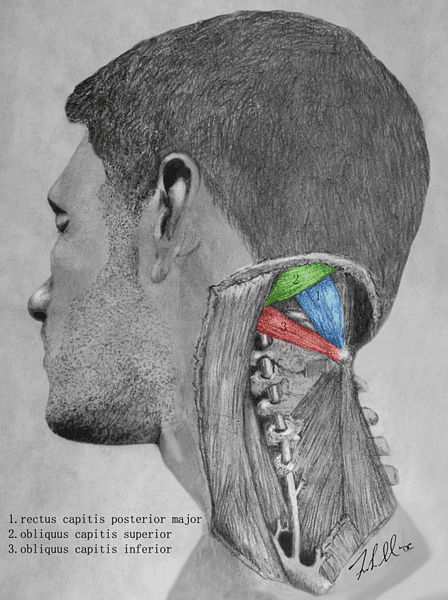
The suboccipitals are four small muscles that are located on either side of the base of your skull. The four muscles are rectus capitis posterior minor (RMAJ), rectus capitis posterior major (RMIN), inferior oblique and superior oblique. The subocciptal muscles are responsible for fine motor control; as well as stabilizing, extending and rotating the head and neck. Smaller muscles like the subocciptials tend to have a lot of sensors, such as muscle spindles that detect the rate in which a muscle changes its length or position. This positional awareness is called proprioception and is often described as your sixth sense. The suboccipitals are so important for propriocetive information that one study found that the inferior oblique and RMAJ had 242 and 98 spindles per gram of muscle tissue, compared to the traps and lats which had 2.2 and 1.4 muscle spindles per gram.
The other proposed mechanism of the suboccipitals is that they have been shown to modulate the tension of the myodural bridge. The myo (muscle – suboccipital) dura (outer most pain sensitive lining covering the brain and spinal cord) bridge is a ligament like structure that attaches the suboccipital muscles to the dura. The bridge provides passive and active anchoring of the spinal cord. It also prevents the dura from buckling inwards when you extend your head. Conversely, it prevents compression of the spinal cord when you bend your head forward. Of the four suboccipital muscles, the RMAJ, RMIN and inferior oblique have all been shown to have their own myodural bridges. It is the job of those muscles to adjust the tension of the bridge (via the stretch reflex), anchoring the spinal dura during changes in head and positioning.
When there is significant trauma to the neck, studies have shown that the cross-sectional area (CSA) of the suboccipitals decreases (atrophy). Reserach has also shown that there is a correlation between the decreased CSA of RMAJ and RMIN in individuals with chronic tension-type headache. The reason for this is following an injury to the neck, the subocciptals alter their function, and lose some of their sensory information and endurance strength capabilities. This affects their ability to anchor the spinal dura during head and neck movements, causing the dura to buckle with neck extension. A reduction of sensory information also alters the gate control of pain.
Tension Headaches and Post-Concussive Symptoms
A recent article published in the American Journal Neuroradiology looked at the CSA of the RMIN in individuals with post concussive symptoms. The researchers found that a smaller CSA was associated with increased symptom severity, longer recovery time, poor verbal memory performance and increased prevalence of headaches. The authors concluded that
‘Given the unique connection of this muscle to the dura, this finding may suggest that pathology of the myodural bridge contributes to symptoms and prognosis in concussed individuals’.
Treatment of Tension Headaches
The initial pharmaceutical Intervention for tension headaches is over the counter pain medication. Pain medication, muscle relaxants, anti-depressants, blood pressure medication and anti-seizure medication may also be prescribed in a preventative, daily nature. Patients should be informed that taking daily medication for headaches can lead to medication overuse headaches.
Therapeutic Interventions for Tension Headaches
For chronic tension-type headaches the Canadian chiropractic association’s clinical practise guidelines (CPG) recommend low force mobilization of the head and neck. The CPG also mentions a high quality study that found spinal manipulative therapy (adjustments) to be effective for chronic tension type-headaches. Kahkeshani and Ward found similar results in their study. They postulated that the myodural bridge provides a mechanical explanation for the efficacy of massage and manipulative treatments with tension and cervicogenic headaches. Other therapeutic interventions include deep neck flexor endurance exercises, as well as subocciptial rehab exercises.
If you have any questions regarding any of the information provided, please visit sportsrehabandwellness.ca.